The side effects of levodopa can be somewhat difficult to distinguish from the many symptoms of the disease itself, since almost everyone with advanced Parkinson’s eventually winds up on one of the levodopa-containing drugs. Nonetheless, common adverse reactions firmly linked to levodopa include dizziness, insomnia, and hypotension (especially after standing up, so-called orthostatic hypotension). But the most obvious and characteristic side effect is dyskinesia. Many people have seen video of Michael J. Fox displaying prominent dyskinesias, and these are commonly misunderstood to be symptoms of the disease itself rather than a drug side effect. Not all patients develop dyskinesias, but most do if they remain on levodopa long enough. (Virtually all young-onset Parkinson’s patients develop dyskinesias, for reasons that are not entirely clear.) Dyskinesias can vary significantly in severity and in the nature of the involuntary movements.
Complicating the picture further, there are at least 2 major patterns for when dyskinesias occur: peak-dose and biphasic. Peak-dose is exactly what it sounds like: dyskinesias are maximally troublesome when the level of levodopa in the body is at a maximum, typically within an hour after the last dose. This pattern makes intuitive sense: at peak dose, there is “too much” dopamine, leading to the involuntary movements; conversely, when the level of levodopa falls, symptoms of the disease itself become problematic, often dramatically so in patients with prominent on-off cycling. The challenge, then, is maintaining levels of levodopa as steady as possible, not too high and not too low. Strategies for achieving this are described here.
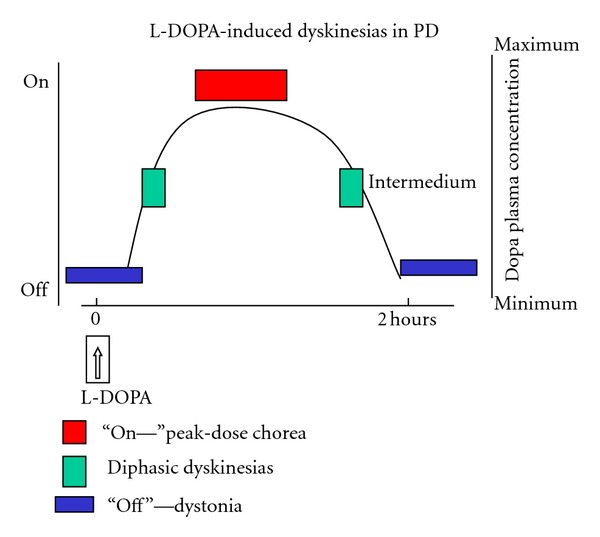
Many patients experience dyskinesia when levodopa levels peak, shortly after taking a levodopa-containing pill (“peak-dose dyskinesia”, red); others experience “diphasic” dyskinesias, which occur when levodopa levodopa levels are changing rapidly (green). Open source image gratefully acknowledged, taken from Clinical Features, Pathophysiology, and Treatment of Levodopa-Induced Dyskinesias in Parkinson’s Disease.
But the existence of biphasic dyskinesias suggests that this straightforward picture may be overly simplistic. Rather than occurring at peak dose, biphasic dyskinesias occur when levodopa levels are rapidly rising or falling, most commonly just before taking a dose and the hour after taking a dose (double your fun!). Regardless of the evident complexity of the underlying biology, the goal remains the same: maintain levodopa levels as steady as possible.
Fear of developing dyskinesias plays a powerful role in patient choices regarding medication. Although evidence supporting the strategy is weak, many patients seek to delay starting on levodopa therapy as long as possible, choosing to use dopamine agonists or MAO-B inhibitors instead, or even forgoing all drug treatment. When prescribed levodopa-based drugs, many patients also try to minimize dosage, sometimes to the extent that their Parkinson’s symptoms are not managed optimally. A simple but interesting study quantified fear of dyskinesia among patients, by asking them (in slightly different words), “Which you rather have, dyskinesia or parkinsonism?” Patients who did not currently have dyskinesias split roughly 50/50, with a slight majority suggesting (astonishingly) that they would rather suffer from the symptoms of Parkinson’s disease than from dyskinesia. Patients who actually had dyskinesia, on the other hand, overwhelmingly preferred to live with dyskinesia than parkinsonism.
