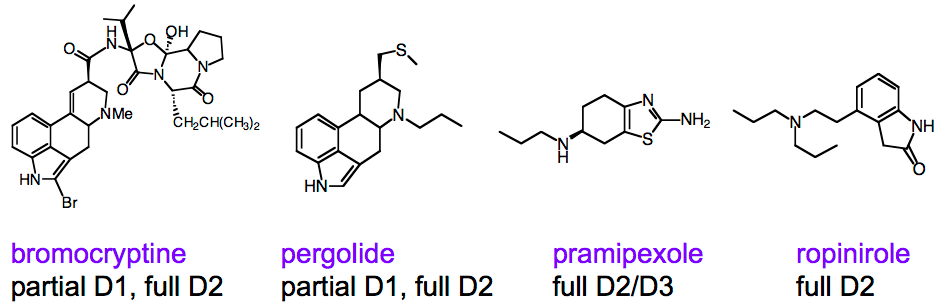
The basic concept of dopamine agonists is to provide a dopamine substitute, that is, a molecule that will bind to the same receptors and exert (roughly) the same effect. There are quite a few compounds in this class, although only a few are widely prescribed. As can be seen in the figure, the resemblance to dopamine is not so obvious, except perhaps if you are a medicinal chemist. Bromocryptine is an example of an older class of dopamine agonists that are derivatives of “ergot” natural products; these are now seldom used for Parkinson’s disease due to side effects. Pramipexole, marketed as Mirapex, is currently the mostly highly prescribed dopamine agonist, and ropinirole, marketed as Requip, is the second most prescribed.
The major advantage of dopamine agonists relative to levodopa is the much more favorable pharmacokinetics. While levodopa is cleared with a half-life of only about an hour, the dopamine agonists have much longer half-lives, over six hours, so that they only need to be dosed 3 times daily. The much more stable blood levels, compared with levodopa, lead to fewer complications of on-off cycling and dyskinesia; on the other hand, dopamine agonists are significantly less effective in managing Parkinson’s symptoms. For this reason and many others, making a fair comparison of the advantages and disadvantages of dopamine agonists vs. levodopa is complex, and has been heavily debated. Some aspects of the debate are discussed elsewhere on this website in Is levodopa toxic? and Fear of levodopa: Does it stop working?. Dopamine agonists were also heavily marketed by pharmaceutical companies as an alternative or adjunctive to levodopa, which of course is not under patent protection. Rightly or wrongly, in practice, dopamine agonists are commonly prescribed to newly diagnosed patients. Eventually, however, essentially all patients transition to or add levodopa-based drugs to achieve adequate management of symptoms.
Recently, evidence has emerged that dopamine agonists can have relatively rare but severely destructive side effects that can be described as “impulse control disorders”: patients who have never been gamblers losing their life savings at casinos, reckless spending or sexual behaviors, etc. (Some of these cases received widespread media attention.) These behaviors had been frequently dismissed as either a consequence of the disease rather than the treatment, or simply as unrelated to Parkinson’s. But patient experiences suggested that the behaviors would frequently end when dopamine agonist treatment was ceased (see, e.g., this study). Several clinical studies [e.g., 1, 2, 3, 4] have now demonstrated, beyond any reasonable doubt, that dopamine agonists cause these side effects. Thus, while a great many patients have used these drugs safely, it is critical that patients and their families be aware of the potential for these relatively rare but extremely destructive side effects.
Why might dopamine agonists cause these effects? Put simply, dopamine agonists are not dopamine. The molecules, while they bind to the same receptors, don’t bind with the same affinity as dopamine or exert the exact same effects; they are not recycled and degraded in the same way as dopamine either. Dopamine signaling in the brain is highly complex, and there isn’t just one receptor for dopamine; rather, there are 5 major receptors, conveniently named D1, D2, D3, D4, and D5. D1 and D5 have somewhat similar roles, as do D2, D3, and D4, and these groups are rather confusingly referred to as “D1-like” and “D2-like” respectively. The various dopamine agonists, and dopamine itself, bind to each of these receptors with different potencies and different degrees of “agonism” (how much downstream signaling is triggered); as might be expected, none of the dopamine agonists match dopamine’s effects. In principle, better understanding of the connection of these side effects to the complex pharmacology could lead to safer and more effective dopamine agonists.
