Approximately 30% of people with Parkinson’s disease have symptoms of orthostatic hypotension, which is defined by a significant drop in blood pressure within a few minutes of standing up. Orthostatic hypotension can be a disabling non-motor symptom because the sudden loss of blood pressure can cause dizziness or even fainting, which can in turn contribute to falls or other injuries. Our understanding of how it results from Parkinson’s disease remains imperfect, but it is clear that Parkinson’s can lead to defects in the nervous system outside the brain, including neurons that control critical functions like blood pressure and heart rate.
Orthostatic hypotension can sometimes be controlled adequately by non-pharmacological approaches, including changes to diet. Several drugs have been used as well, but are often only partially successful. The idea of droxidopa is to directly correct the molecular defect that causes orthostatic hypotension, specifically the failure of norepinephrine (also known as noradrenaline) signaling to properly adjust blood pressure after standing. The simple act of standing requires a rapid physiological response in the cardiovascular system, primarily constriction of the blood vessels in the lower body to avoid blood pooling in the legs with a resulting drop in blood pressure. Norepinephrine is responsible for triggering the constriction of the blood vessels, and in neurogenic orthostatic hypotension (i.e., when the condition is caused by neurological problems, such as Parkinson’s disease), the norepinephrine response is insufficient.
Interestingly, norepinephrine is chemically very similar to dopamine, the primary neurotransmitter that is deficient in Parkinson’s disease, differing only by the addition of a hydroxyl (OH) group. Norepinephine itself can be administered by injection, but this is not a practical approach to treating orthostatic hypotension. This suggests a therapeutic approach highly analogous to the use of levodopa to correct for the deficiency in dopamine: administer a pro-drug that can be administered orally and then get converted into norepinephrine in the body. This is precisely how droxidopa works; in fact, the same enzyme that converts levodopa into dopamine also converts droxidopa into norepinephrine. Droxidopa is also known as L-dihydroxyphenylserine, L-DOPS, which emphasizes the similarity to L-DOPA.
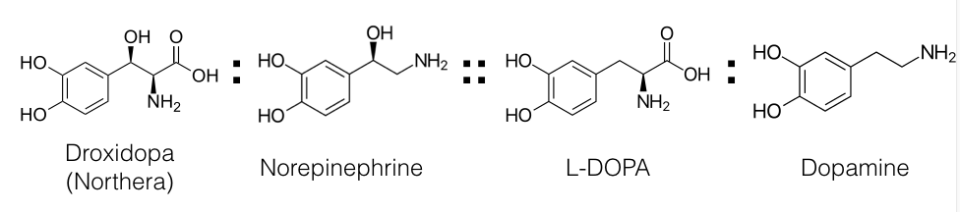
A chemical analogy
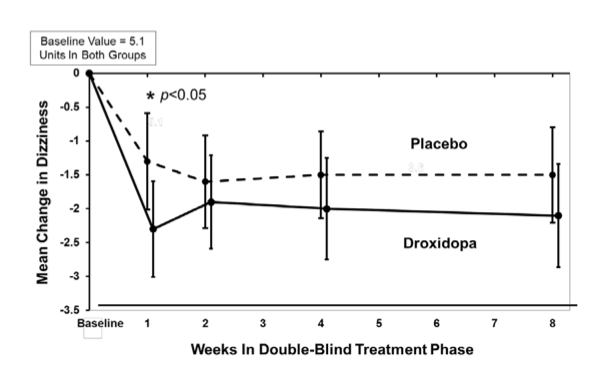
In 2014, the FDA granted accelerated approval to droxidopa based on a series of rather short clinical trials. The longest placebo-controlled trial was only 8 weeks long, and even in this trial, droxidopa was only demonstrated to have a statistically significant benefit up to 2 weeks, in part due to a large placebo effect.
The relatively small effect of the drug, combined with lack of strong evidence for long-term efficacy, has led to a great deal of criticism of the FDA decision. The positive decision appears to have been driven by droxidopa’s potential to address, even partially, an under-treated and very serious symptom of Parkinson’s disease, and by droxidopa’s relatively clean safety profile. The most important side effect, with a black box warning, is the risk of supine hypertension. That is, increasing the too-low blood pressure when standing can also cause blood pressure to increase when lying down, with all of the health consequences associated with hypertension in general. The long-term safety and efficacy of droxidopa are currently being studied in a so-called phase 4 (post-approval) clinical study; results do not appear to be available yet.
