Since Parkinson’s is caused by degeneration of dopamine-producing neurons, leading to insufficient dopamine, the first obvious therapeutic strategy would be to give patients dopamine. In fact, dopamine can be used as a drug, but not for Parkinson’s. There are two basic problems: (1) administering dopamine orally (by mouth) leads to nasty side effects, and (2) dopamine in the blood doesn’t enter the brain to any significant extent (it doesn’t “cross the blood-brain barrier“).
The solution to this problem is to instead administer L-DOPA, which is the chemical from which dopamine is created in your brain, as discussed here. When used in drugs, L-DOPA is called levodopa.
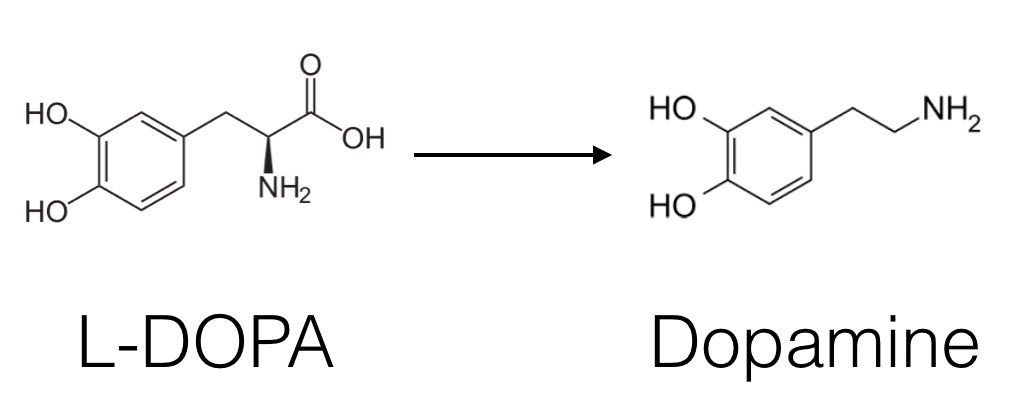
L-DOPA does get across the blood-brain barrier, with the assistance of a transporter called LAT1, which is normally used to get certain amino acids, such as tyrosine and tryptophan, from your blood into your brain. Once in the brain, L-DOPA can be quickly converted to dopamine, by an enzyme called aromatic amino acid decarboxylase, AADC. This is an example of a prodrug strategy, in which you administer a drug that is converted by the body into the actual active molecule.
But there is a problem: L-DOPA can also be converted into dopamine before it gets to the brain, by the same AADC enzyme. That’s not good, because the extra dopamine in your bloodstream has side effects, like causing your heart to race, and because the brain gets less L-DOPA and thus the drug is less effective. For this reason, L-DOPA is almost never administered alone; it is instead administered as a combination drug with at least one other ingredient, carbidopa, which blocks AADC from converting L-DOPA into dopamine. And here is the coolest trick: carbidopa does not get into the brain. So it only blocks conversion of L-DOPA to dopamine outside the brain, which is exactly what we want.
